
Building on spectacular scientific achievements, the rich world’s vaccine response to the pandemic within its borders has been (with notable exceptions) commendable. But the response of the international community has been mystifyingly myopic and unconscionably delinquent. We’re headed toward global “vaccine apartheid.”
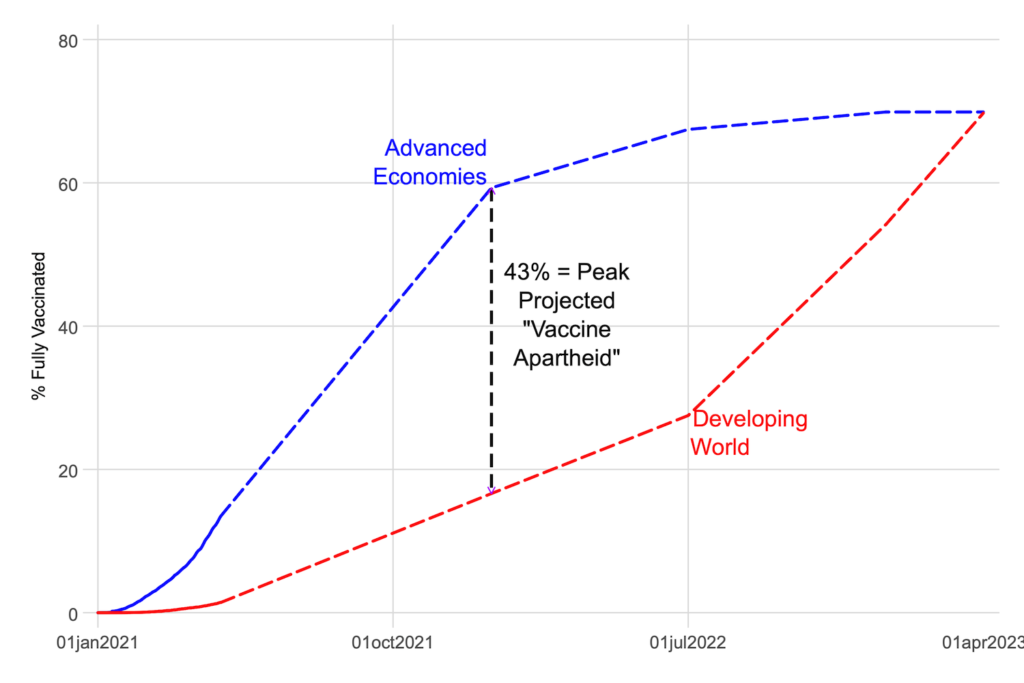
Figure 1 plots an index of this global vaccine apartheid, measuring the difference in vaccination rates between rich and poor countries. We use actual vaccination rates through April 2021, then aggregate national projections from the Economist Intelligence Unit going forward. On current policies—production and financing—this index will continue rising and peak toward the end of this year (with differences in rates at close to 50 percentage points). Optimistically, only in 2023 will this disparity be eliminated and global herd immunity be close to being achieved.
Figure 1. An index of global vaccine apartheid
Disparities are likely to get much worse, long before they get better
The consequences of this apartheid are playing out heart-wrenchingly in Brazil, India and perhaps also soon in other places. Make no mistake. This apartheid was inherent to the conception and design of policy, a feature not a bug.
Manufacturing capacity was planned to supply Western markets almost exclusively, with a proprietary, intellectual property (IP)-based approach guaranteed to limit its spread. And money from donors was derisively small and never close to enough to buy—or even signal to producers that there was sufficient demand for—vaccine doses to cover much of the developing world.
No doubt, developing country governments—India, in particular—have mismanaged their own domestic vaccine response, such that not all blame for the emerging vaccine apartheid rests on rich-country shoulders. India erected barriers to entry of foreign vaccine producers, failed to make purchase orders, and created uncertainty for domestic production as well. Though as the pandemic continues to grow and spread and supplies remain essentially fixed, it’s unclear if more international purchasing by India would have been anything but a zero-sum reallocation globally. Our focus here is on escaping that zero-sum math.
Remedial action is imperative and urgent to minimize the humanitarian disaster unfolding around the world. We propose a multi-pronged response, spearheaded by the Biden administration, which should use its convening power to bring together developing-country leaders and pharmaceutical industry representatives at a summit to hammer out a strategy. The broad contours of this strategy would involve actions by governments of rich nations, middle-income nations, international institutions, philanthropies, and pharmaceutical companies to boost supply and financing.
Current supply can be augmented by two sets of actors aimed at two sets of vaccine technologies.
Augmenting supply of mRNA vaccines requires US political leadership
Regardless of the IP regime, no developing country, and perhaps no firm anywhere in the world, has the technical wherewithal to produce the Pfizer or Moderna mRNA vaccines without significant technical assistance from these companies. If (and we emphasize if) there can be progress on expanding manufacturing of these vaccines, the US government along with other governments will have to incentivize and force western pharmaceutical companies to share their technology and knowhow via voluntary licensing to similar companies in the developing world. The incentivization could take the form of guaranteeing commercial or near-commercial royalty rates by the international community. The global social costs of vaccines even with commercial royalty is trivial compared to the global social benefits.
The reality is that the US already used coercion in the COVID pandemic, invoking the Defence Production Act several times to increase domestic production capacity in various ways. Whereas the US action was zero sum, we need coercion to secure a non-zero sum outcome, namely a global expansion of capacity. That means the coercion would have to be applied collectively by the international community and targeted at the collective of all vaccine producers.
A summit convened by the Biden administration would provide an impetus and a forum for the drawing up of a detailed plan between western pharmaceutical companies, especially Pfizer, Moderna, and Johnson and Johnson, and their counterparts—supervised and under-written by relevant governments to boost global supply of vaccines.
Some middle-income countries already have technical ability to increase supply of other vaccines through joint compulsory licensing—they should use it
Reliance on voluntary actions by the US government or pharmaceutical companies may not be enough, as the status quo shows. Developing countries must have some levers of their own—for intrinsic reasons of seeking to augment capacity and for instrumental reasons as a threat against western pharmaceutical companies.
Unlike with the mRNA vaccines, compulsory licensing of non-replicating viral vector vaccines can be credibly implemented by advanced developing countries such as Brazil, Argentina, India, Thailand, and South Africa because two conditions are met. Companies located there already have the knowhow to manufacture the vaccine (as with the AstraZeneca vaccine in Brazil and India) or developed the technology domestically (as with the Bharat Biotech vaccine in India). Second, they have a critical mass of pharmaceutical companies with manufacturing capability who would be the recipient of compulsory licenses.
The US should bless the use of compulsory licensing, which does not require an intellectual property waiver from the WTO
Having the technical capability is one thing, but there is also the international legal regime to consider. Nothing in current international rules prevents such compulsory licences especially when used to cater to domestic needs. Nothing in current rules should prevent compulsory licensing from being used to exporting vaccines and catering to the needs of other countries. In fact, that was the purpose of the agreement in the World Trade Organization (WTO) during the AIDS crisis.
Despite this, individual countries might still be fearful of either retaliatory action by the US or the reputational costs of issuing compulsory licenses (deterring future investors). These could be addressed in three ways. Instead of any one country issuing compulsory licensing, perhaps a group of middle income nations can act together to do so.
To signal that their seriousness and responsibility, developing countries should make good faith efforts to secure commitments on voluntary licensing from Western pharmaceutical companies before issuing compulsory licensing; committing to near-commercial terms for compulsory licenses would also signal good faith by clarifying that the motive is production not expropriation. Another sign of good faith would be if, e.g., India were to apply compulsory licensing not just to foreign vaccines, but also to domestically developed technology such as Bharat Biotech.
For their part, governments of the US and Europe should forswear any recourse to legal proceedings (say, in the WTO or under free trade agreements) against countries that use compulsory licensing. Supporting the IP waiver that developing countries have asked for would be desirable but a simpler alternative could be an immediate WTO agreement or a political declaration to a “standstill” on any action relating to vaccines and the pandemic.
In some ways, the arguments on both sides about the TRIPS waiver (i.e., the proposal by developing countries to suspend the WTO’s IP protections for COVID vaccines) are odd. Developing countries are over-obsessed with the need for the TRIPS waiver, almost conceding that existing rules do not allow compulsory licensing and such departures from IP in the case of epidemics and pandemics. On the other hand, the pro-IP crowd such as the US and Bill Gates is disingenuous in claiming that waiving IP is irrelevant to augmenting capacity. If that were so, what is the harm in suspending IP, which at worst might be inconsequential and at best could help expand production? The crescendoing global pandemic puts the onus on IP advocates to make the case to restrict potential vaccine supply in any way.
So, a global summit with US backing could be the forum where the joint compulsory licensing is announced with the political WTO declaration on a legal standstill on COVID-related actions (for a limited period of necessary) being the imprimatur for the action by developing nations.
Since the aim is augmenting global capacity, as Chad Bown and Tom Bollyky argue, no country should apply restrictions on the sale or exports of any of the inputs that go into vaccine production. Increasing global capacity will put pressure on input supply, creating cost puch for vaccine prices, but the international community should be willing to accept these higher costs.
On the demand side, the global vaccine response requires a dramatically larger, simpler financial commitment
The international community, via COVAX, should take seriously its role of providing global public goods. In estimating the funding of COVAX, two principles should be decisive. First, vaccine quantities should be adequate to reach herd immunity in all the “AMC91” countries designated by COVAX, and 2022 and 2023 as possible deadlines would be inadequate. That means generating 5.4 billion doses as quickly as possible.
The second relates to prices. In rich countries, all citizens are getting free vaccines. It would be ethically unconscionable if that principle did not apply to much poorer people in much poorer countries. Every person in the world must receive free vaccines as soon as they can be produced, a benefit that all citizens in rich countries are experiencing today. Vaccines are a textbook case where huge positive externalities necessitate free public provision—at both the national and global level. Granted, some upper-middle income countries such as Brazil and Mexico are surely able to finance part of this cost for their citizens. But given the scale of the global benefit from all countries achieving herd immunity, it would be self-defeating to ask the AMC91 countries (primarily low- and lower-middle income) to pay anything for vaccines. The international community must foot the bill.
Taking seriously the current estimates of global vaccine roll out, that in turn means COVAX should be funded by grants to the tune of somewhere between $75-$150 billion, depending upon the cost of a vaccine dose. At the high end, that would represent less than 0.4 percent of combined G7 GDP, or just 3.8 percent of what G7 countries spent on discretionary fiscal stimulus in response to the COVID crisis in 2020, and would be a fraction of the decline in GDP of poor countries and rich countries’ GDP that would be prevented by having the poor fully vaccinated. And if philanthropies shouldered a share of that resource-raising, that would probably also represent a small share of their endowments.
G7 governments can easily afford this price tag, and there is no need to complicate the financing arrangements. Recently, Gordon Brown and others have rightly and eloquently called for raising more money to address the vaccination gap. They propose sophisticated mechanisms such as vaccine bonds, underwriting risk guarantees, and the like. In our view, funding to eliminate the vaccine apartheid should be simple: contributions from rich country governments as grants to cover the purchase of vaccines for distribution in poor countries. Vaccine bonds, IMF special drawing rights, and other kinds of funny money generate uncertainty at a moment when both the world and vaccine producers need clear assurance of robust demand.
The funding of COVAX should also factor in a new dimension in addition to its mandate to make advance purchases on behalf of poor nations. It must also have the resources to pay for the knowhow and technology for voluntary and compulsory licensing. As discussed above, increasing capacity will require incentivizing the pharmaceutical companies. The attendant costs must not be borne by developing country governments or their citizens.
We are agnostic about whether a new institution should be created for implementing our proposed strategy or whether COVAX should be re-hauled.
The United States has a choice between two forms of soft power: Technological superiority and global apartheid or human immunity and Pax Americana
Aiming to reassert or regain its global role in the aftermath of the Trump era, the Biden administration is caught between two forces. On the one hand, there is the inevitable loss in technological and economic supremacy with China’s unavoidable ascendancy. On the other, there is the opportunity to burnish its global image both to make up for the lost Trump years and to highlight the contrast with the soft power-undermining turn that China has taken under Xi Jinping.
Its scientific achievements in rapid vaccine development are tempting the US (abetted by the pharmaceutical industry) to exploit the pandemic to seek and maintain technological superiority relative to China. If it succumbs, it is not likely to favour the global vaccine strategy we have proposed because that would entail the sharing of technology.
Treating the pandemic response as an arms race would lead to a great loss of American soft power. The remarks of the State Department spokesman on April 22nd, asserting that the US should not just prioritize its domestic vaccination drive over the rest of the world, but that other nations should be grateful, grated on the world and diminished US global standing considerably. Reports that pharmaceutical companies are lobbying the US government to prevent life-saving mRNA technology from falling into the hands of the Chinese or Russians has stoked the world’s worst fears about America’s intentions.
Visibly leading the charge to vaccinate the world, with significant political and financial commitments, offers the US the chance to regain considerable soft power.
So, the choice for the Biden administration is clear: seek to maintain technological superiority (possibly ephemeral because there are no guarantees that it can be maintained) vis-à-vis China, accept the status quo of global vaccine apartheid, and diminish itself in the eyes of the world.
Alternatively, it could convene the Global Vaccine Summit immediately to augment global vaccine supply itself, bless the effort of other countries to do so themselves, and help raise the resources required to finance this strategy and resurrect, even if only as possibility, Pax Americana.
Global vaccine apartheid, or a step toward Pax Americana? The choice is yours, President Biden.
This blog was originally published by the Centre for Global Development here

